Using Mobile Tethering for sharing data across devices: application in rural eye screening
Dr George Kong PhD1, Dr Jonathan Kam MBBS1
1Royal Victorian Eye and Ear Hospital, Melbourne, Australia
Corresponding Author: georgekong008@gmail.com
Journal MTM 1:3:40-45, 2012
DOI:10.7309/jmtm.21
Background: Eye screening programs have been effective in reducing the burden of eye diseases in the developing world. Most use paper recording systems which are prone to misplacement and are inefficient for auditing purposes. Digital data collection via mobile devices may prove more efficient, but reliable strategies information sharing between devices in rural settings remain an issue. This paper examines the speed and range of use of Mobile Tethering technology to synchronize data across devices, and hence the suitability of such devices in the eye screening setting.
Methods: The data synchronization feature of eyePatients software for iPhone and iPad was tested using an Apple iPhone 4 as the central router, with Mobile Tethering activated. Apple iPad 2 devices were connected to the wireless local area networks (WiFi) generated by the iPhone 4. The linear range of data synchronization and the effect of corners and barriers on synchronization were tested.
Results: Synchronization was rapid, taking between 1.0-1.5 seconds to complete when linear distance was within 30 meters. Beyond 34 meters considerable slowing was noted and no successful connections were able to be established beyond 40 meters. A single corner had no statistically significant effect on the maximum range of a single tether connection, but two corners or a door barrier had a small but statistically significant reduction on range.
Conclusion: Mobile Tethering provides a reliable and fast connection between multiple devices that can be used for the synchronization of large amounts of data required for eye screening purposes.
Introduction
The introduction of the tethering function on iPhone (Apple, Cupertino, California, USA) and other smart phone devices has opened up opportunities for changing the way data can be collected and shared in the clinical setting. Very few studies have examined the potentials of using such technology in clinical screening programs in rural and remote areas. Clinical screening programs such as HIV screening and eye screening have been effective in reducing the burden of diseases in the most needed parts of the world 1-51. Murthy GV, Ellwein LB, Gupta S, et al. A population-based eye survey of older adults in a rural district of Rajasthan: II. Outcomes of cataract surgery. Ophthalmology. 2001;108(4): 686-92.
2. Nirmalan PK, Robin AL, Katz J, et al. Risk factors for age related cataract in a rural population of southern India: the Aravind Comprehensive Eye Study. Br J Ophthalmol. 2004;88(8): 989-94.
3. Zhao J, Jia L, Sui R and Ellwein LB. Prevalence of blindness and cataract surgery in Shunyi County, China. Am J Ophthalmol. 1998;126(4): 506-14.
4. Zhang M, Wu J, Li L, et al. Impact of cataract screening outreach in rural China. Invest Ophthalmol Vis Sci.51(1): 110-4.
5. Wand H and Ramjee G. The relationship between age of coital debut and HIV seroprevalence among women in Durban, South Africa: a cohort study. BMJ Open.2: e000285.. For instance, eye screening programs travel to rural areas and only stay in a particular location for short durations (usually days) to screen large numbers of patients, typically a few hundred patients per day, for treatable eye disease such as cataracts, pterygium, and diabetic retinopathy. 22. Nirmalan PK, Robin AL, Katz J, et al. Risk factors for age related cataract in a rural population of southern India: the Aravind Comprehensive Eye Study. Br J Ophthalmol. 2004;88(8): 989-94.
,6-86. Hautala N, Hyytinen P, Saarela V, et al. A mobile eye unit for screening of diabetic retinopathy and follow-up of glaucoma in remote locations in northern Finland. Acta Ophthalmol. 2009;87(8): 912-3.
7. Wedner SH, Ross DA, Balira R, Kaji L and Foster A. Prevalence of eye diseases in primary school children in a rural area of Tanzania. Br J Ophthalmol. 2000;84(11): 1291-7.
8. Congdon NG, Quigley HA, Hung PT, Wang TH and Ho TC. Screening techniques for angle-closure glaucoma in rural Taiwan. Acta Ophthalmol Scand. 1996;74(2): 113-9.. Therefore they depend on heavily on efficient and reliable data collection.
Patients going through eye screening process would normally undergo registration of information, nursing assessment, medical assessment and counselling. Upon determining that the patient requires and consents to medical treatment, the patient’s information is kept with the team and arrangements would then be made for the patient to return on a surgery day for treatment. This process in most eye screening teams is currently performed using a paper recording system. The disadvantages of a paper based system is that it is prone to record misplacement or damage and needs to have details manually re-entered into a computer system for auditing purposes. With the recent availability of large numbers of affordable and portable mobile devices, there is increasing enthusiasm for the use of such devices in clinical settings 9-119. Dala-Ali BM, Lloyd MA and Al-Abed Y. The uses of the iPhone for surgeons. Surgeon.9(1): 44-8.
10. Bastawrous A, Cheeseman RC and Kumar A. iPhones for eye surgeons. Eye (Lond).26(3): 343-54.
11. Perera C. The Evolution of E-Health – Mobile Technology and mHealth. Journal MTM. 2012;1(1): 1-2.. The advantages of electronic data collection in the field include clear and legible documentation, eliminating need for repeat manual entry and eliminating risk of misplacement of paper documents.
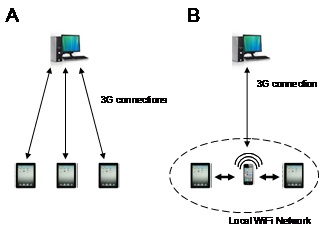
Figure 1 – Models of data sharing between mobile devices (A) Each mobile device shares data with central server via mobile connection, (B) Mobile devices shares a working set of data via local WiFi Network and final dataset is sent to central server at the completion of screening through mobile connection.
The main challenge of the digital data collection is for several devices situated in different rooms of a screening station to share the same patient information. There are essentially two potential strategies for tackling this issue. Method one is to have each device connect to and then share data on a central server several kilometres away via 3G (3rd generation mobile telecommunications) mobile network connection (Figure 1A). This method is disadvantaged by the fact that 3G mobile networks are often unreliably slow in rural areas, making this paradigm potentially too slow to handle the large throughput required. The alternative paradigm is to have the mobile devices on the field communicate with each other directly. This has been made possible recently with the introduction of the Mobile Tethering technology. Mobile Tethering is a technology whereby a smart phone can acting as a wireless local area networks (WiFi) router by broadcasting signal for a local WiFi network. Devices connected to the WiFi network will be assigned a unique IP (internet protocol) address, through which data can be transmitted directly (Figure 1B). The data collected by the devices can then be transferred or E-mailed back to central server at the completion of the screening day.
Smart phones on the market capable of Mobile Tethering include Apple iPhone 4, iPhone 4S and some Android based mobile phones (Android, Inc., Palo Alto, California, USA). There are also increasing number of medical related mobile Applications (Apps) that utilizes this feature, including eyePatients (George Kong Softwares, Melbourne, Australia) on Apple AppStore ®.
This paper examines the speed and range of use of Mobile Tethering technology to synchronize data across devices, and hence the suitability of such device in the eye screening setting.
Methods
Systems Setup
An Apple iPhone 4 running iOS 4.3.3 operating system (Apple, California) was used as the central router. Mobile Tethering option was turned on under the Mobile Hotspot option within Mobile Settings. Once Mobile Tethering was turned on, Apple iPad 2 devices were connected to the wireless local area networks (WiFi) generated by the iPhone 4 by selecting the iPhone 4 name in the searchable Networks. The login process involved entering the pre-assigned password on the iPhone 4 Hotspot option.
Data synchronization was tested on the iPad with iPad App eyePatients and on iPhone with the App eyePatientsMobile (George Kong Softwares, Melbourne, Australia). eyePatients and eyePatientsMobile Apps are clinical data management Apps designed to help eye care clinicians including ophthalmologists, ophthalmology residents, optometrists and students in recording patient data, including visual acuity and intraocular pressure data. These Apps were acquired from Apple AppStore. The selection of these Apps for use in this paper was purely for the purpose of testing the proposed model in the paper and is not an endorsement of the Apps. Data synchronization was performed under the Synchronization module within the eyePatients and eyePatientsMobile Apps. Under the synchronization module, the local IP address of the mobile device is displayed, which is used by other mobile devices for connection to the device.
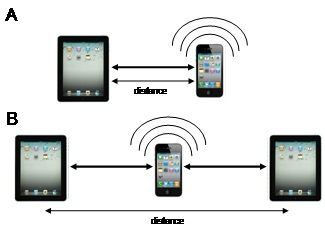
Figure 2 – Testing linear range of data synchronization on Mobile Tethering network: (A) for single tether connection, (B) for two tether connections.
Testing linear range of data synchronization
The linear range of a single tether connection was tested along a straight indoor corridor, between an iPad 2 and an iPhone 4 (Figure 2 A). The two devices were placed at increasing linear distances from each other starting from 2 meters and subsequently in 2 meter intervals. The distances were measured with tape measure and positions marked prior to starting testing to ensure accurate straight measurements down to nearest centimetre. Ten patient data records (approximately 6 kilobyte of data) were entered in the iPad 2 device for each synchronization test. The duration of synchronization (from start of pressing synchronization button to message showing synchronization complete) was recorded with a digital timer. Three synchronizations events were performed at each position until loss of communication is reached such that synchronization is not able to be completed. The point at which communication is lost was tested five times by reducing the distance back within range by 4 meters and re-extend the distance out at 1 meter intervals until communication is lost again. The total combined linear range of two tethering connections was tested similarly, this time using two iPad 2 devices with the central iPhone 4 in the centre (Figure 2B). The two iPad 2 devices were placed with increasing linear distances away from the central iPhone 4, starting from 2 meters (therefore total distance of 4) and increase in 2 meter intervals. Synchronization testing was conducted in a similar manner as described above.
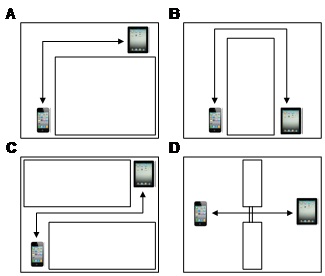
Figure 3 – Testing effect of corners and barrier to data synchronization on Mobile Tether connection, (A) Single corner (B) Two corners scenario 1 (C) Two corners scenario 2 (D) Barrier with one wooden door.
Testing the effect of corners and barriers
As the stations of an eye screening program are not usually aligned in a linear fashion but instead in separate rooms, it is necessary to understand whether Tethering signal is affected by bends in the path or barriers. These were tested on a single tether connection between an iPad 2 and an iPhone 4 (Figure 3). To test around single corner (Figure 3A), the mobile devices were placed at equal distances from a corner formed by two concrete walls. Distances from the corner were increased symmetrically from 2 meters onwards in 2 meter steps. To test around two corners, two scenarios were performed, scenario 1 (Figure 3B) involved having a fixed inter-corner distance of 4 meters and altering the distance of mobile device from their closest corner. Scenario 2 (Figure 3C) involved performing synchronization testing with different inter-corner distances. To test the effect of wooden door barrier, the two testing devices were placed at increasing distances away from a wooden door mid-way in the path between them.
Statistics
Comparisons of measurements were performed with using two-sided Student’s T-test with alpha level of 0.05.
Results
Speed and linear range
Synchronization of 10 records using the eyePatients App was rapid, taking between 1.0-1.7 seconds to complete when linear distance was within 30 meters. Beyond 34 meters considerable slowing was noted in the initiation of data connection (Table 1 and Figure 4). No successful connections were able to be established beyond 40 meters (Table 1). By having the tethering iPhone as the central point, two iPad 2 were able to synchronize across even greater linear distance (Table 1). The maximum distance for functional synchronization is approximately double the distance for single tethering connection.
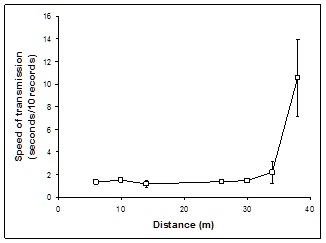
Figure 4 – Speed of transmission of 10 data records at various linear distances on a single tether connection.
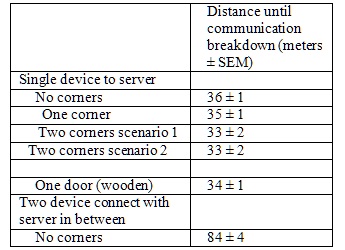
Table 1: Maximum range distance for tethering connection arrangements. (n=5)
Effects of corners and barriers
Single corner had no statistically significant effect on the maximum range of a single tether connection (Table 1). For both two corner scenarios, maximum range of a single tether connection was reduced to 33 m (p=0.01, p<0.025 with Bonferroni correction). The effect of a door barrier on maximum linear range was small (approximately loss of 2 m) but statistically significant (p=0.01).
Discussion
This paper examined the speed and range of use of Mobile Tethering technology to synchronize data across mobile devices. Knowledge of the capabilities and limitations is important for designing the physical layout of eye screening stations. This study demonstrates that using Mobile Tethering, a reliable and fast connection can be established between multiple devices for synchronization of large number of data records required for eye screening purpose.
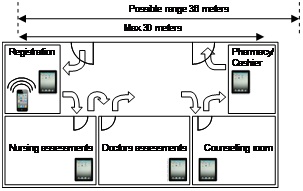
Figure 5 – An example of physical layout of mobile devices in an eye screening station.
The range of connection covers a considerable distance, up to 30 meters reliably for single tethering connection with no corners or barrier. Even when the connection needs to bend across two corners or through a wooden door barrier, the maximum range was reduced minimally by approximately 2 meters. The actual distance between two iPad devices can be greater (up to 80 m) by having the iPhone device broadcasting WiFi signals in the centre. The range of transmission is greater than Blue Tooth connection which is typically of the range of 5-10 meters. This capability of range allows for much flexible designs for physical layouts of mobile devices in eye screening stations for digital recording of patient information. For example, a 30 meter length community hall could be divided as shown in Figure 5 into logical stations for eye screening. A longer up to 60 m linear camp setup can also be arranged with the Tethering iPhone device placed centrally (Figure 6). The Mobile Tethering model outlined in this paper could potentially be useful for screening programs in other disciplines (such as for otolaryngology and cardiology). Clinical data management Apps for general medicine currently available which allows data sharing over WiFi network include My Medical App (Hyrax Inc.) and MedicalNotesHD (George Kong Softwares, Melbourne, Australia).
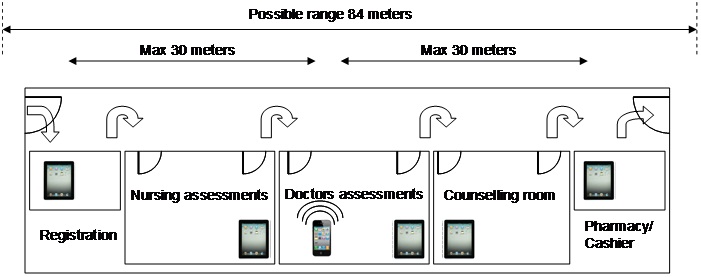
Figure 6 – An alternative example of physical layout of mobile devices in an eye screening station with centrally placed WiFi broadcasting device.
There are some limitations to the Mobile Tethering technology, firstly most smart phone devices limit the maximum number of devices that can be connected to its WiFi network (For iPhone 4 the maximum is 5). Secondly, some Mobile Network providers requires that there has to be some mobile connectivity for the smart phones to generate a WiFi Hotspot network, therefore limiting the use of this paradigm in very remote locations without any mobile connectivity. Thirdly, tethering is a high battery consuming feature; therefore the central tethering iPhone will need to be charged regularly to continue to function. Lastly, WiFi Hostspot network can potentially be influenced by environmental factors such as proximity to high voltage power sources and storms.
This study is not a head-to-head comparison with the alternative model in which each mobile device connects to a distant server via mobile connectivity. However, the alternative model is expected to perform less favourably as it is limited by unreliable slow mobile connectivity in rural areas. It is also counter intuitive that data that needs to be shared between devices in close proximity needs to connect first to a server hundreds of kilometres away. Future studies will involve comparison of various models in head-to-head trials. Lastly we note that WiFi broadcast capabilities is not restricted to smart phones, certain lap-top computer models are also capable of broadcasting WiFi network, in which case the same design paradigm proposed in this paper will also apply.
Conclusion
In conclusion, this study shows that using mobile tethering, reliable and efficient connections can be established between multiple devices for synchronization of data. We found the application of this technology useful in the setting of rural eye screening.
References
1. Murthy GV, Ellwein LB, Gupta S, et al. A population-based eye survey of older adults in a rural district of Rajasthan: II. Outcomes of cataract surgery. Ophthalmology. 2001;108(4): 686-92. ![]()
2. Nirmalan PK, Robin AL, Katz J, et al. Risk factors for age related cataract in a rural population of southern India: the Aravind Comprehensive Eye Study. Br J Ophthalmol. 2004;88(8): 989-94. ![]()
3. Zhao J, Jia L, Sui R and Ellwein LB. Prevalence of blindness and cataract surgery in Shunyi County, China. Am J Ophthalmol. 1998;126(4): 506-14. ![]()
4. Zhang M, Wu J, Li L, et al. Impact of cataract screening outreach in rural China. Invest Ophthalmol Vis Sci.51(1): 110-4. ![]()
5. Wand H and Ramjee G. The relationship between age of coital debut and HIV seroprevalence among women in Durban, South Africa: a cohort study. BMJ Open.2: e000285.
6. Hautala N, Hyytinen P, Saarela V, et al. A mobile eye unit for screening of diabetic retinopathy and follow-up of glaucoma in remote locations in northern Finland. Acta Ophthalmol. 2009;87(8): 912-3. ![]()
7. Wedner SH, Ross DA, Balira R, Kaji L and Foster A. Prevalence of eye diseases in primary school children in a rural area of Tanzania. Br J Ophthalmol. 2000;84(11): 1291-7. ![]()
8. Congdon NG, Quigley HA, Hung PT, Wang TH and Ho TC. Screening techniques for angle-closure glaucoma in rural Taiwan. Acta Ophthalmol Scand. 1996;74(2): 113-9. ![]()
9. Dala-Ali BM, Lloyd MA and Al-Abed Y. The uses of the iPhone for surgeons. Surgeon.9(1): 44-8. ![]()
10. Bastawrous A, Cheeseman RC and Kumar A. iPhones for eye surgeons. Eye (Lond).26(3): 343-54. ![]()
11. Perera C. The Evolution of E-Health – Mobile Technology and mHealth. Journal MTM. 2012;1(1): 1-2. ![]()
