Preliminary study on use of mobile phone by interns to answer pager messages
Dhara N. Perera1
1Dr. MBBS, Bsc. (Hons), House Medical Officer – Eastern Health, Victoria; James Cook University, Queensland, Australia
Corresponding Author: dharanalika@gmail.com
Journal MTM 2:2:24–30, 2013
http://dx.doi.org/10.7309/jmtm.2.2.6
Background: Improved communications within the healthcare sector is imperative to enabling increased clinical efficiency and enhanced quality of patient care. Mobile phone use has been demonstrated to enhance clinical practice by improving communication between physicians, junior medical staff and other healthcare members.
Aims: This study aims to assess use of personal mobile phones to answer pager messages (use versus non-use) among Intern medical officers.
Methods: A literature search was performed. A survey instrument was designed to identify intern medical officers who used their mobile phones to answer pager messages and those who did not. 12 intern medical officers were surveyed. Verbal consent was obtained. Following completion of the instrument, when necessary, participants were asked to clarify their comments.
Results: Among the 12 intern medical officers, 8 intern medical officers (67%) used their personal mobile phone to answer pager messages. Main reasons highlighted were convenience, hospital phone accessibility and time-saving. Reasons for non-use by 33% participants were to keep work and private calls separate and not wishing to pay for work-related calls.
Conclusions: Those junior medical officers who answered pager messages using their mobile phone found it beneficial due to increased productivity. Those who did not chose to do so due to privacy and cost. Further validation with larger scale randomized control studies in this field are required.
Introduction
Mobile technology is a rapidly advancing field with widespread uses demonstrated in the healthcare network, particularly in relation to improving communications within the hospital system. Efficient and timely communications within the hospital is imperative to enable delivery of timely services and quality care to patients. This is dependent on a constant stream of communication between all levels of staff including medical, nursing and allied health staff on a daily basis1–3. Whilst mobile technology continues to advance, there is limited evidence demonstrating improvements in communications within hospitals and in clinical outcomes.
The benefits described in the literature include perceived faster communication amongst clinicians, more efficacious time usage, reduction in response time and response errors, improved quality and efficiency of communication between physicians1–7.
The effects of poor communication systems and patterns of communication behaviours within different hospital sectors (e.g. in general medical wards and emergency departments) have been investigated locally and globally in several quantitative studies1,2,4,8. The researchers have mainly adopted observational methods, mixed-method studies involving surveys, monitoring activities and interview based methodologies, collectively highlighting problems such as communication interruptions affecting (doctors and nurses equally) and consequentially resulting in communication errors translating into adverse clinical outcomes. Hence these studies demonstrate the adverse impact that ineffective clinical communications can have on delivery of quality care by causing preventable errors3. The studies performed are small-scale level involving students, doctors and nursing staff.
Several studies highlight the lack of efficiency in current pager messaging systems, which are still the main mode of communication within most hospital networks1,2,8. The lack of efficiency in the paging systems has seemingly led to an increased trend towards adopting Smartphone use, Webpaging to Smartphones, and messaging via email2,4,7,8.
Quantitative studies have shown improved perceptions of communication and some improvement in communication metrics, whilst the qualitative studies demonstrated improvements in efficiency of communications. However, despite the increasing number of studies, there is a paucity of high quality quantitative studies identified2,8. In a clinical study, Ramesh et al. demonstrated that among 116 medical students, junior medical officers and Consultants, 67% used their phones for work related calls and 47% whilst attending patients6. Haroon et al. validated these findings by demonstrating a 98.3% rate of mobile phone use among doctors for work purposes4. Another benefit found was quicker contact of medical staff by hospital telephone operators and perceived efficiency in communication by doctors themselves6. Additionally, a significant reduction in the number of fixed-line calls received in hospital wards, reduced response time and response errors with Smartphone use compared with pagers and were strongly preferred over pagers by junior medical officers due to and improvements in perceived quality and efficiency of communication1.
The potential disadvantages highlighted were a lack of reliability, potential breach in confidentiality, contamination of mobile phone devices and potential electromagnetic interference (EMI) in with other electromagnetic devices (e.g. automated external defibrillators and electrocardiogram machines)9–13. Therefore in the hospital setting one needs to maximise the benefits while taking necessary steps to avoid collateral damage.
As a medical intern a significant proportion of time is spent answering, sending and receiving numerous pager calls on a daily basis, of varying urgency. In the traditional hospital systems, junior doctors are paged and expected to answer using the hospital telephones available. An important limitation preventing answering pager messages promptly is a lack of easily accessible/available hospital phones. Hence both junior and senior medical officers of various disciplines are known to use their personal mobile phones for work related calls to facilitate time effective communication within the hospital system. This action helps reduce time-wasted waiting/searching for hospital phones, alleviates stress and provides an easier mode of communication.
In view of a paucity of information in relation to junior medical staff using their personal mobile phones to answer pager messages, a small-scale preliminary study was performed on a small cohort of intern medical officers working at a regional level hospital in Victoria.
Methods
A PUBMED search was performed which revealed 155 articles. The search results were screened for articles relevant to the current study, which revealed 13 studies on the use of mobile phones in hospitals by medical staff. Keywords used were mobile phones in hospitals, Smartphones, Pager, mobile phone, intern medical officer and efficiency.
A small-scale descriptive study was performed on a group of intern medical officers in order to determine current mobile phone practices to answer pager messages and identification of factors for non-use at Ballarat Health Services (BHS). The survey instrument used is given in the Appendix. The survey was administered to a group of 12 out of the 28 intern medical officers who were chosen based on their availability and accessibility. Survey was explained and verbal consent obtained. Participants were requested to score each item form 0-10 on a linear scale where 0 was not at all a reason and 10 being very important A post-survey interview was conducted primarily to clarify some of the information provided. All of the doctors who were requested to fill the form agreed to participate. The survey instrument was designed following discussion with colleagues and an assumption was made of its face validity.
Results
With the exception of one doctor the other 11 used the mobile phone on a regular basis. Eight doctors (67%) used their personal mobile phone in the hospital to answer their pager.
Table 1 summarises the advantages as noted by those who used their phones. There were two important reasons demonstrated i.e. time-saving and accessibility of a phone.

Table 1: Rationale for regular use of mobile phones
Figure 1 illustrates the individual response scores for the above, combining time-saving and convenience as one unit and availability and accessibility of phones as one unit. For the sake of clarity when a 0 was scored for any item we assigned a score of 1.
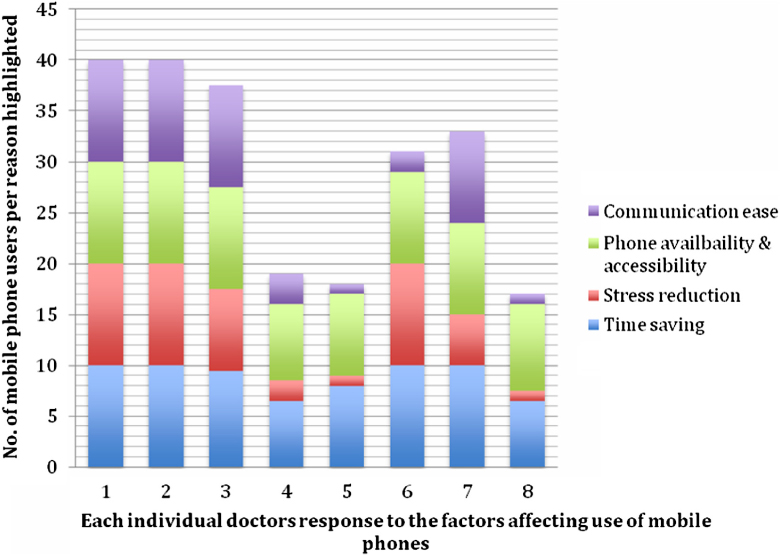
Figure 1: Individual responses for those who used their phone to answer paged calls
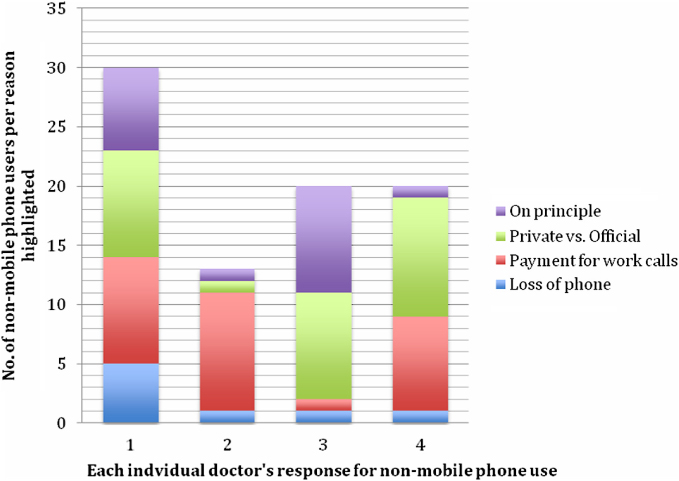
Figure 2: Individual responses for each reason among those who did not use their phone to answer the pager
Those who did not use a mobile phone to answer their pager, felt that they should not have to pay for work related calls and preferred to keep their private phones for personal use only (see Table 2).
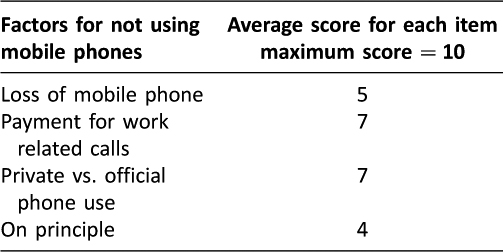
Table 2: Reasons for not using mobile phones
On interview of participants among the comments revealed issues related to mobility, and the benefit noted was that they could attend to other tasks and move around the ward whilst answering a pager message.
The primary reasons identified for regular use of their mobile phone were convenience, time-saving, not having to wait for phones to become available/ search for a phone on the ward, easier mode of communication with senior staff (e.g. Registrar) and facilitates mobility between wards, operating theatres and within the ward e.g. to bedside of patient whilst speaking to senior if required.
The four individuals who did not use their personal mobile phones to answer pager calls stated that they wish to keep their private phones separate from work related activity and felt that they should not be paying out of their pocket for official duties. One individual also commented that it was a matter of principle.
Discussion
Taking advantage of mobile phones to improve communications has been widely demonstrated in both quantitative and qualitative studies to increase efficiency, reduce clinical errors and adverse effects, improve quality of patient care, enhance communication between physicians and ability to deal with a myriad tasks simultaneously, particularly at a junior level2–48. The present small-scale quantitative study was performed in order to ascertain the feasibility of a larger scale evaluation in a similar setting. The study sample was limited by time and resources constraints faced by the author.
The benefits demonstrated in the present study were similar to the findings in the study by Haroon et al. where all but one of the 60 doctors in the study reported using their mobile phone to answer pager messages, and for private for communication and paid privately4. Similarly, in the present study it was demonstrated that the majority of junior doctors used their personal mobile phones for work related calls as they found it beneficial. The main reasons were convenience, easy accessibility and availability of their phone and the reduced wastage of time (Figure 1). However, there is a dependency on adequate network coverage within the hospital premises to successfully utilise ones mobile phone which maybe variable. This is particularly associated with some phone carriers especially in rural or remote areas. Those who did not use their phones indicated that it was due to wanting to separate official and personal communications and also not wanting to pay for hospital related calls.
In view of the challenges associated with communication systems within hospitals, multiple alternative interventions have been explored by various research groups. Whilst some of the challenges have been overcome by introduction of Smartphones in certain hospitals e.g. in Canada, no clear resolution has been reached. Other traditional hospitals continue to use the traditional pager messaging system for communication. Some of the unintended issues found with Smartphone use was an increase in communication interruptions.3,12 Lo et al. aptly described disadvantages of pager systems – a lack of information causing frustration for the receiver with provision of only a call back numbers and little or no context to the message leading to difficulty in prioritization as well as causing interruption to patient care and workflow2. This can be a significant deterrent to clinical outcomes.
Whilst individuals are applauded for their principles in not using their personal phones for hospital work, the advantages of using a mobile phone seem to outweigh the disadvantages or perceived losses. Those who mentioned cost as a reason for not using their mobile phone need to take into account that work related calls are tax deductible. Additionally the time saving factor would most likely increase productivity thus making work more rewarding.
In a much larger study by Wu et al. (2011), where Smartphones were supplied and used for communication between staff, the benefits were replicated, although a drawback identified was significant increase in interruptions to work due to the messages themselves1. Other negatives were variability in urgency, lack of reliability and unprofessional conduct in terms of lack of confidentiality whilst using this mode of communication.12,13 However, this situation had arisen in the context of an attempt to replace the paging system with use of smart phones.
Use of the mobile phone is likely to increase productivity and reduce time wasted on waiting around for a land phone to answer pagers. Furthermore if the individual who sent the page is not immediately available, having the mobile phone will allow the intern to attend to the numerous other duties, instead of waiting by the land phone awaiting the return call.
In view of the potential for increased work place productivity, provision of mobile phones to intern medical officers maybe a cost-effective measure. When pager calls are answered promptly and dealt with, this becomes more cost-effective for the medical workforce by enabling ward-based work to occur within the rostered hours. Hence less overtime claims. If there are concerns regarding potential misuse of the facility, calling limitations could be placed (call barring).
It maybe postulated that provision of a work mobile phone would also reduce the workload on the busy hospital telephone operators in cases where an extension number is not provided.
Overall this study has helped to elucidate some of the factors that make communication via mobile phones favourable among clinicians and medical officers. Although a small-scale study it significantly contributes to the existing pool of evidence that highlight the advantages associated with Smartphone/ mobile phone usage in the clinical setting. Some of the limitations identified in this study are selection bias associated with administering of survey to colleagues who were readily accessible and the small sample size.
Concluding remarks
The findings of the current study supports the literature suggesting enhanced inter-professional communications with mobile phone usage within the hospital network. The primary reasons promoting regular mobile phone use identified were time-saving in the context of having to multi-task and reduce time-wasted searching for a landline or waiting for a phone to become available and convenience among the junior medical staff.
Time wasted on waiting for hospital phones would then be reflected in an increased number of overtime hours claimed, which translates as an extra cost incurred by the hospital healthcare sector.
Finally, in order for formal implementation of improved communication methods within the hospitals globally, further high quality large-scale studies and randomized control trials on use of mobile phones to answer pager messages need to be conducted. Additionally in order to ascertain the value of providing intern medical officers with mobile telephones, the attitudes of the health care practitioners and allied health members need to be further examined as well as the impact on delivery of quality clinical care. Potential benefits and problems need to be further evaluated to clearly identify whether the benefits outweigh the harm.
References
1. Wu R, Rossos P, Tran K, Quan S, Reeves S, Lo V, Wong B, Cheung M, Morra D. An Evaluation of the Use of Smartphones to Communicate Between Clinicians: A Mixed-Methods Study. Journal of Medical Internet Research. [Internet]. 2011 Jul-Sep [cited 2013 Feb]; 13(3):e59
2. Lo V, Wu R.C, Morra D, Lee L, Reeves S. The use of smartphones in general and internal medicine units: A boon or a bane to the promotion of interprofessional collaboration? Journal of Interprofessional care. 2012;26:276-82. ![]()
3. Coiera E.W, Jayasuriya R.A, Hardy J, Bannan A, Thorpe M.E.C. Communication loads on clinical staff in the emergency department. Medical Journal of Australia. 2002;176:415-8.
4. Haroon M, Yasin F, Eckel R, Walker F. Perceptions and attitudes of hospital staff toward paging system and the use of mobile phones. International Journal of Technology Assessment In Health Care. 2010;26(4):377-81. ![]()
5. Wu R, Wodajo F. The Smartphone in Medicine: A Review of Current and Potential Use Among Physicians and Students. Journal of Medical Internet Research. [Internet]. 2012 Sep 27 [cited 2013 Feb];14(5):e128. ![]()
6. Ramesh J, Carter A.O, Campbell, M.H, Gibbons N, Powlett C, Moseley Sr H, Lewis D, Carter T. Use of mobile phones by medical staff at Queen Elizabeth Hospital, Barbados: evidence for both benefit and harm. Journal of Hospital Infection [Internet]. 2008 Aug 12 [cited Feb 2013]; 70:160-5. Available from: www.sciencedirect.com
7. Coiera E, Tombs V. Communication behaviours in a hospital setting: an observational study. British Medical Journal. 1998;316:673-6.
8. Wu, R.C, Tran K, Lo V, O’Leary K.J, Morra D, Quan, S.D, Perrier L. Effects of clinical communication interventions in hospitals: A systematic review of information and communication technology adoptions for improved communication between clinicians. International Journal of Medical Informatics. 2012;81:723-32.
9. Klein A.A, Djaiani G.N. Mobile phones in the hospital – past, present and future. Anaesthesia. 2003;58:353-7.
10. Baranchuk A, Kang J, Shaw C, et al. Electromagnetic Interference of Communication Devices on ECG Machines. Clinical Cardiology. [Internet]. 2009 [cited Feb 2013];32:588-92. ![]()
11. Trigano A, Blandeau O, Dale C, Wong M, Wiart J. Clinical testing of cellular phone ringing interference with automated external defibrillators. Resuscitation. 2006;71:391-4. ![]()
12. Wu R.C, Lo V, Morra D, Wong B.M, Sargeant R, Locke K, Cavalcanti R, Quan S.D, Rossos P, Tran K, Cheung M. The intended and unintended consequences of communication systems on general internal medicine inpatient care delivery: a prospective observational case study of five teaching hospitals. Journal of American Medical Informatics Association. [Internet]. 2013 Jan 26 [cited Feb 2013];0:1-12. Available from:
13. Barton A.J. The Use of Short Message Service in Hospitals. Information Technology and the Clinical Nurse Specialist. 2012; 300-1.
The use of personal mobile phone to answer the pager
As an intern I found that using my mobile to answer the pager was very helpful. There were others who felt they should not. At the end of the intern year I thought of asking around regarding the matter.
Do you use a mobile phone on a regular basis Yes/No
Do you use your mobile phone in the Hospital to answer your pager Yes/No
Please answer the following if you use the phone to answer the pager
giving a score of 0 if not a reason at all and 10 being extremely important
Convenience ………………………………………………………………………………………………….
Time saving ………………………………………………………………………………………………….
Causes me less stress ………………………………………………………………………………………………….
I do not have to wait for a phone to become available ………………………………………………………………………………………………….
I do not have to go looking for a phone ………………………………………………………………………………………………….
I can speak with the person who paged me directly ………………………………………………………………………………………………….
Any comments /other benefits ………………………………………………………………………………………………….
………………………………………………………………………………………………….
Please answer the following if you do not use the phone to answer the pager
giving a score of 0 if not a reason at all and 10 being extremely important
I might lose the phone ………………………………………………………………………………………………….
I should not be paying for Hospital related calls ………………………………………………………………………………………………….
I like to keep my private phone separate from work ………………………………………………………………………………………………….
On principle ………………………………………………………………………………………………….
Any other disadvantages ………………………………………………………………………………………………….
………………………………………………………………………………………………….
Any further comments
Optional: Your Name/email
