Comparison of Mid-Sternum and Center of Mass Accelerometry to Force Plate Measures for the Assessment of Standing Balance
Ryan Z. Amick, PhD1 , Nils A. Hakansson, PhD2, David M. Jorgensen2, Jeremy A. Patterson, PhD3, Michael J. Jorgensen, PhD2
1College of Innovation Design, Wichita State University, Wichita, KS, United States
2Department of Biomedical Engineering, Wichita State University, Wichita, KS, United States
3Department of Human Performance Studies, Wichita State University, Wichita, KS, United States
Corresponding Author: nils.hakansson@wichita.edu
Background: Accelerometric assessment of balance is typically conducted from lower back locations approximating the center of mass (COM).
Aims: Because placement of accelerometers at the approximate COM may not always be practical, the purpose of this study was to determine if significant differences exist between acceleration measures recorded from the mid-sternum, COM, and center of pressure (COP).
Methods: Data were collected from 25 subjects (13 male; 22.4 ± 3.3 years) as they performed 30 sec trials of bipedal standing and single leg standing. Accelerations were simultaneously recorded via tri-axial accelerometers attached at the mid-sternum and approximate COM (i.e., over L3), and by force plate. Signals were tilt corrected and root mean squared (RMS) values of the accelerations were calculated. Repeated measures ANOVA were performed to determine if differences exist between accelerometer measurement locations as a function of stance and accelerometer location.
Results: No significant differences in mean RMS acceleration between the accelerometer locations were observed during bipedal standing in the anterior-posterior (p = 0.140), medial-lateral (p=0.170), or vertical directions (p = 0.270). For the single leg stance, significant differences were observed between measurement locations in the anterior-posterior (p < 0.001), medial-lateral (p = 0.002), and vertical directions (p < 0.001).
Conclusion: Trunk accelerations recorded from above the center of mass may provide useful measures for identifying those with reduced postural control.
Keywords: balance, accelerometers, force plate, center of mass, postural control
Introduction
Human balance is a complex and multi-dimensional process that allows for the maintenance of a specific posture, or postures, while executing any number of different tasks. These tasks can vary from simple activities of daily living such as sitting upright or static standing, to more complex skilled activities executed while performing work duties or recreational activities. Our ability to perform this wide range of activities is dependent upon our capacity to coordinate and control various components of multiple intrinsic systems which contribute to the process of maintaining balance.1 These include biomechanical, motor, and sensory components which are further influenced by task demands, environmental constraints, and individual capabilities.1–5
The quantitative assessment of standing balance has traditionally been accomplished with the use of a single force plate. Here, the amplitude and velocity of center of pressure (COP) excursions are measured in the anterior-posterior and medial-lateral directions. An increase in these values is then generally interpreted as the individual demonstrating poor balance.6 Force plates have been reported to be valid and reliable for the assessment of standing balance.7 However, the use of COP excursion measures has been questioned by some as it may indicate a change in postural control strategy as opposed to poor postural control.8–10 An alternative method for quantitatively measuring balance is with the use of accelerometers.
For the measurement of balance, accelerometers are typically placed along the lumbar spine at the approximate location of the whole body center of mass (COM). When attached here, accelerometers have demonstrated fair to excellent correlation to force plate balance assessments.6,11–13 A number of authors further report that, during both bipedal and single leg balance assessments, acceleration patterns recorded from the estimated COM behave similarly to COP acceleration patterns measured via a force plate.6,12,14 It has additionally been argued that, for the assessment of balance, the accelerations recorded from the COM may provide a better indicator of postural control than do COP measures.8
Another potential site of sensor attachment for balance assessment is the sternum. In an investigation of gait and balance in those with Huntington’s disease, Dalton and colleagues15 attached a single tri-axial accelerometer to the sternum just inferior to the suprasternal notch. Balance was assessed utilizing four Rhomberg balance tests including feet together with eyes open and closed, and feet apart, eyes open and closed. Results indicated that acceleration data recorded from the sternum could differentiate between pre-symptomatic and symptomatic Huntington’s disease patients. Janssen and colleagues16 additionally attached accelerometers to the sternum to assess balance during sit-to-stand movements. Subjects performed sit-to-stand movements on a force plate with an accelerometer placed over the sternum. These investigators reported a correlation coefficient of 0.77 between force plate and acceleration data. However, the authors stated that the purpose of the study was to quantify trunk movements during the sit-to-stand test, and not to use the attachment site data as a corollary to balance as assessed by center of mass variables.16 Recent investigations have investigated the use of a tri-axial accelerometer built into a mobile consumer electronics device for the purpose of providing a quantitative clinical balance assessment.17,18 The device is held at the level of the mid-sternum for ease of placement, and measures trunk accelerations that result from the balance control strategy employed by the subject. However, it is currently unknown how trunk kinematics recorded at the mid-sternum level for the purpose of assessing balance compares to those recorded from the more accepted measurement locations, such as the estimated COM or from a force plate.
Given the previous research, a question arises as to whether similarities or correlations exist between accelerations measured at the mid-sternum and other measurement locations such as the estimated center of mass and at a force plate. An answer to this question could provide insight into understanding various instrumented balance assessment methods and clarify whether findings from one study can be compared to those of another using different accelerometer placement. Therefore, the objective of this study was to determine if differences exist in balance measures (i.e., accelerations) recorded with tri-axial accelerometers attached at the mid-sternum level and that measured at other commonly used sites, including the approximate COM, and measured with a force plate. It is hypothesized that accelerations measured from the mid-sternum location will be significantly different than accelerations measured from the COM and COP.
Methods
A total of 25 subjects (13 male, 12 female; aged 22.4± 3.3 years) volunteered to participate in this study (Table 1). All participants were university graduate and undergraduate students free from any condition or injury that may have limited their standing balance. All methods and procedures were approved by the Wichita State University Institutional Review Board for Human Subjects. An Informed Consent form describing the nature of the testing to be completed, as well as exclusion criteria, was provided to all participants upon arrival to the testing facility. Testing procedures were then explained to all participants and exclusion criteria confirmed verbally. Participants were excluded if they reported any current or pre-existing neurological, musculoskeletal, visual, vestibular, or other conditions that may have altered their ability to balance normally. Upon receiving approved informed consent, demographic and anthropometric measures were recorded.
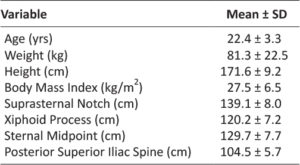
Table 1: Subject Demographic and Anthropometric Data.
Anthropometric measures were collected using aGPM calibrated anthropometer (Siber-Hegner, Switzer-land). Anthropometric measures recorded included standing height, height from the floor of the suprasternal notch, height from the floor of the xiphoid process, and height from the floor of the third lumbar vertebrae as determined by palpation.19 Height from the floor of the suprasternal notch and xiphoid process were averaged to determine the sternal mid-point. Standing height and weight were used to calculate each subject’s body mass index (BMI). For all measures, subjects did not wear shoes.
Acceleration measures were recorded utilizing two Zephyr BioHarness 3 (BH3) devices (Zephyr Technology Corp., Annapolis, MD, USA). The BH3 device is a compact monitoring system that is designed for mobile physiological monitoring. The device includes a MEMS tri-axial accelerometer capable of measuring accelerations of ±16g,20 an inclinometer to measure tilt in the X-Z plane, and an elastic strap to secure the device to the user. The first BH3 device was placed on the chest at the calculated height of the sternal midpoint, and measured accelerations of the upper trunk. The second BH3 device was placed on the lumbar spine at the level of the third lumbar vertebrae (L3), determined by palpation, as the approximate whole body COM.COP movements were recorded using a multi-axis force plate (AMTI BP600600) (Advanced Mechanical Technology, Inc., Watertown, MA, USA) (Figures 1 and 2).

Figure 1: Bipedal stance condition with subject standing on force plate and tri-axial accelerometers attached at the mid-sternum and L3.

Figure 2: Single leg stance condition with subject standing on force plate and tri-axial accelerometers attached at the mid-sternum and L3.
After recording all demographic and anthropometric information, the BH3 devices were placed at the sternal midpoint and L3 locations with an elastic strap fit with a custom receptacle to secure and orient the device (Figure 1 and 2). The mid-sternum BH3 device was oriented in a manner that accelerations in the positive X-direction corresponded with anterior movement, and accelerations in the positive Y-direction corresponded with lateral movement to the right. The L3 BH3 device was oriented such that accelerations in the positive X-direction corresponded with posterior movement, and accelerations in the positive Y-direction corresponded with lateral movement to the left. The elastic strap for each BH3 device was positioned around the subject’s torso so that the accelerometer Y-direction was as closely aligned with the transverse plane as possible. After the BH3 devices were attached, subjects were instructed to stand on the force plate.
Accelerometer and force plate ground reaction force data normalized to body mass (i.e., center of pressure standard deviations)21,22 were collected simultaneously while subjects performed one trial each of two Romberg stances, which included bipedal standing with feet together and eyes closed, followed by dominant leg single leg stance with eyes open. Each stance was performed without shoes for a period of 30 seconds, and subjects rested for a period of no less than two minutes between stance conditions. For each test, subjects were instructed to stand quietly as accelerometer and force plate signals were measured at 50Hz and 1000Hz, respectively. Accelerometer data was transmitted wirelessly via Bluetooth to an external computer for storage. Force plate signals were time synchronized to match the 50Hz accelerometer data. Subjects performed a familiarization trial prior to performing each stance. The middle 15-second window of each trial was used in the RMS calculations.21
All acceleration data was post-processed in a custom MATLAB program (The Math Works, Inc., Natick, MA, USA). Accelerations from the L3 BH3 device were transformed so that the positive and negative anterior-posterior, medial-lateral, and vertical directions corresponded to the mid-sternum BH3 device and the force plate. Anterior-posterior acceleration data from both BH3 devices were corrected for tilt in the X-Z plane using the respective BH3 anterior inclinometer measures. Subsequently, medial-lateral acceleration data were corrected for tilt in the Y-Zplane.9,23 After processing, the acceleration root mean square (RMS) in the anterior-posterior, medial-lateral, and vertical directions were calculated for each measurement location.
The statistical analysis consisted of a two-way repeated measures Analysis of Variance (ANOVA), performed separately for each of the three directions (i.e., anterior-posterior, medial-lateral, vertical). For each ANOVA, the independent variables consisted of the location of acceleration measurement (mid-sternum, L3, force plate) and the stance (bipedal, single leg), and the dependent variable was the RMS of the acceleration. Significant main effects were assessed by the Tukey Honest Significant Difference post-hoc test. Significant interactions were assessed by the least significant difference post-hoc test, with a Bonferroni adjustment for the number of comparisons, where comparisons of interest included the mid-sternum to the L3 and force plate locations. Significance was indicated using α=0.05. All statistical analyses were performed with the use of SAS Version 9.1 (Cary, NC).
Results
The mean RMS acceleration values measured at L3 were higher than those for the mid-sternum and force plate in the anterior-posterior (0.700 vs. 0.462 and 0.064m/s2, respectively) and medial-lateral (0.703 vs. 0.352 and 0.069m/s2, respectively) directions for single leg stance and in the medial-lateral direction for bipedal stance (0.794 vs. 0.236 and 0.058m/s2, respectively). The mean RMS acceleration values measured in the anterior–posterior and medial–lateral directions at the force plate for both bipedal and single leg stance were lower than those measured at both the mid-sternum and L3. In the vertical direction, the force plate mean RMS acceleration values were highest for both bipedal and single leg stance. The resulting mean and standard deviation of the RMS accelerations as a function of direction (anterior-posterior, medial-lateral, vertical), stance (bipedal, single leg) and measurement location (mid-sternum, L3, force plate) are shown in Table 2.
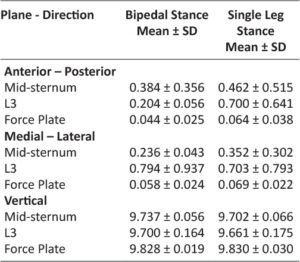
Table 2: Mean (SD) RMS of acceleration measured at the mid-sternum, L3, and mean RMS of center of pressure acceleration measured at the force plate, as a function of the anterior-posterior, medial-lateral vertical planes, for the bipedal stance (feet side by side) and dominant leg single leg stance.
Statistical analyses showed the RMS accelerations were different as a function of stance and location, depending on the direction of the acceleration. In the anterior-posterior direction, there were significant main effects of measurement location (p < 0.001), stance (p = 0.002) and a significant location×stance interaction (p < 0.001). Post-hoc analysis of the significant interaction indicated that for the single leg stance, the mean RMS acceleration measured at the mid-sternum was significantly different than that measured at L3 (p = 0.006) and the force plate (p < 0.001). For the bipedal stance, the mean RMS acceleration at the mid-sternum was significantly different than that measured at the force plate (p = 0.002), but not significantly different from the L3 measurements (p = 0.034) (see Figure 3). In the medial-lateral direction, the RMS acceleration varied significantly as a function of measurement location (p < 0.001), but not by stance (p = 0.851), nor was there a significant interaction (p = 0.260). The post-hoc test on the significant location effect found that the RMS acceleration at the mid-sternum was significantly different from that measured at L3 and the force plate (see Figure 4). In the vertical direction, the RMS acceleration varied significantly as a function of measurement location (p < 0.001), but not as a function of stance (p = 0.155), nor was there a significant interaction (p = 0.422). The follow-up post-hoc test indicated that the RMS acceleration measured at the mid-sternum was significantly different than the RMS acceleration measured at the force plate, but not at the L3 level (see Figure 5).

Figure 3: Mean RMS acceleration in the anterior-posterior plane as a function of measurement location and stance. Solid horizontal line indicates conditions that were not significantly different from each other.
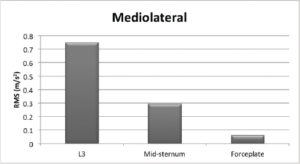
Figure 4: Mean RMS acceleration in the medial-lateral plane as a function of measurement location. Solid horizontal line indicates conditions that were not significantly different from each other.
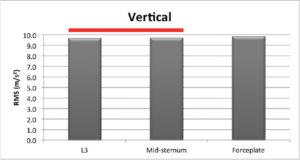
Figure 5: Mean RMS acceleration in the vertical direction as a function of measurement location. Solid horizontal line indicates conditions that were not significantly different from each other.
Discussion
Because accelerometer placement on the body in balance studies varies and because the correlation between balance measures from the chest and other body locations has not been widely reported, the objective of this study was to investigate the balance measures of tri-axial accelerometers attached at the mid-sternum and the estimated COM. The second objective was to examine the balance measures recorded at the mid-sternum and a force plate. One finding from this study was that the balance measures from the two tri-axial accelerometers exhibited differences for both bipedal and single leg stance conditions. Another finding was that balance measures from the mid-sternum accelerometer differed from the force plate for both the bipedal and the single leg stance conditions. The interpretation and importance of these findings are discussed below.
The results for bipedal stance identified statistical differences in mean RMS accelerations in the medial-lateral direction but not the anterior-posterior direction. In a similar study, Mancini and colleagues reported that accelerometer signals recorded from the estimated COM behaved similarly to signals obtained from an accelerometer placed at the C7 vertebra during quiet bipedal stance in both the anterior-posterior and medial-lateral directions.12 The difference in the medial-lateral acceleration results between our study and that of Mancini and colleagues may be due to the bipedal stance width; subjects in our study stood with their feet together. This foot arrangement yields a narrow base of support in the medial-lateral direction, which has been shown to increase medial-lateral movements.24 Additionally, bipedal corrections of medial-lateral sway involve shifting weight between the feet to compensate for COM motion.8 COM motion in the frontal plane will require a concomitant motion by the torso, and therefore mid-sternum, in the opposite direction to maintain the COM over the base of support.
The significant differences in mean accelerations observed in the anterior-posterior and medial-lateral directions between measurement sites during single-leg standing were likely the result of subjects utilizing a combined ankle and hip strategy for maintaining balance. Traditionally the ankle strategy is considered as the primary strategy, particularly with younger subjects.25 In the ankle strategy, the center of mass is manipulated through torques applied primarily at the ankle joint, requiring that the upper and lower body move in unison, similar to an inverted pendulum, as the center of mass is manipulated. Under this scenario, linear accelerations would increase in proportion to the distance from the axis of rotation, the ankle. However, our results indicate larger magnitude accelerations at L3 relative to the mid-sternum in both the anterior-posterior and medial-lateral directions, implying the hip strategy may have been used. With the hip strategy, the center of mass is manipulated through torques applied primarily at the hip joints, causing the upper and lower body to move in opposite directions as the center of mass is manipulated. Additionally, the ankle strategy is generally limited in the medial-lateral direction due to torque generation limitations of the ankle invertors and evertors.8
Comparisons between the acceleration measures at the mid sternum and the force plate indicated differences for both bipedal and single leg stance conditions in the anterior-posterior, medial-lateral, and vertical directions. In the anterior-posterior and the medial-lateral directions, the significant differences in mean accelerations may have been the result of flexion and extension at the hip which coordinated the movement of the trunk relative to the COM.5 The force plate did not record the larger accelerations as the hip strategy creates a compensatory horizontal shear force exerted against the support surface which acts to decelerate the center of mass to control balance.5,26–28 In the vertical direction, significant differences were observed between the mid-sternum and force plate locations. This is likely the result of the hip strategy and the height of the accelerometers above the force plate. As compensatory anterior-posterior and medial-lateral movements of the upper and lower body are made in an effort to control balance, the vertical positions of the accelerometers will change to a greater extent than the whole body center of mass, which is reflected by the force plate acceleration measurement.
A discussion of the study methods is warranted to provide context to the results. The sample population consisted of students recruited from the WSU. These students were also free of injuries or other conditions that could have adversely affected their standing balance and increased the magnitude of the measured accelerations. As a result, the findings may not be generalizable to the larger population. The bipedal stance condition had subjects stand with feet together. The close proximity of the feet resulted in a narrow base of support that could have yielded different acceleration measures than had the feet been placed further apart. Also, this study was conducted in a laboratory setting with few visual and auditory distractions, which may limit the generalizability of these findings with regards to less controlled environments.
Conclusion
Overall, the results of this study indicate that, for those with normal balance, the choice between mid-sternum and L3 measurement locations may be of little consequence. However, as indicated by the differences between the mid-sternum and force plate measurement locations, bipedal and single leg balance measurements recorded at the mid-sternum may provide valuable information with regard to the amount of trunk movement required for a subject to maintain balance. This is further supported by the overall increased anterior-posterior and medial-lateral mean acceleration at the mid-sternum when compared to the force plate. Additionally, the mid-sternum location was able to identify a change in vertical position with trunk movement. The vertical component could potentially be an indication of increased postural instability. This information could prove useful when considering the potential use of MEMS tri-axial accelerometers built into many consumer electronics devices. These devices could be positioned against the mid-sternum location, allowing for the accelerator to capture larger variations in postural sway.
Funding
None
Conflict of Interest
There are no potential conflicts of interests, including financial arrangements, organizational affiliations, or other relationships that may constitute a conflict of interest regarding the submitted work.
References
1. Rose DJ. Balance, Posture, and Locomotion. In: Spirduso WW, Francis KL, MacRae PG, eds. Physical Dimensions of Aging. 2nd ed. Champaign, IL: Human Kinetics; 2005.
2. Shumway-Cook A, Woollacott MH. Motor Control. Theory and practical applications. 4 ed: Lippincott Williams & Wilkins; 2001.
3. Berg K. Balance and its measure in the elderly: a review. Physiother. Can. 1989;41(5):240–246.
4. Horak FB. Postural orientation and equilibrium: what do we need to know about neural control of balance to prevent falls? Age Ageing. 2006;35(suppl 2):ii7–ii11.
5. Horak FB. Clinical measurement of postural control in adults. Phys. Ther. 1987;67(12):1881–1885.
6. Adlerton A-K, Moritz U, Moe-Nilssen R. Force plate and accelerometer measures for evaluating the effect of muscle fatigue on postural control during one-legged stance. Physiother. Res. Int. 2003;8(4):187–199.
7. Goldie PA, Bach TM, Evans OM. Force platform measures for evaluating postural control- Reliability and validity. Arch. Phys. Med. Rehabil. 1989;70(7):510–517.
8. Winter DA. Human balance and posture control during standing and walking. Gait Posture. 1995;3(4):193–214.
9. Moe-Nilssen R. Test-retest reliability of trunk accelerometry during standing and walking. Arch. Phys. Med. Rehabil. 1998;79(11):1377–1385.
10. Panzer VP, Bandinelli S, Hallett M. Biomechanical assessment of quiet standing and changes associated with aging. Arch. Phys. Med. Rehabil. 1995;76(2):151–157.
11. Whitney SL, Roche JL, Marchetti GF, et al. A comparison of accelerometry and center of pressure measures during computerized dynamic posturography: Ameasure of balance. Gait Posture. 2011;33:549–599.
12. Mancini M, Rocchi L, Cappello A, Chiari L. Comparison of wearable inertial devices and force plates for stance posture measurements. Gait Posture. 2008;28:S31.
13. Lindemann U, Moe-Nilssen R, Nicolai SE, Becker C, Chiari L. Assessment of balance in unsupported standing with elderly inpatients by force plate and accelerometers. Aging Clin. Exp. Res. 2012;24(1):37.
14. Mayagoitia RE, Lötters JC, Veltink PH, Hermens H. Standing balance evaluation using a triaxial accelerometer. Gait Posture. 2002;16(1):55–59.
15. Dalton A, Khalil H, Busse M, Rosser A, van Deursen R, ÓLaighin G. Analysis of gait and balance through a single triaxial accelerometer in presymptomatic and symptomatic Huntington’s disease. Gait Posture. 2013.
16. Janssen W, Kulcu D, Horemans H, Stam HJ, Bussmann J. Sensitivity of accelerometry to assess balance control during sit-to-stand movement. Neural Systems and Rehabilitation Engineering, IEEE Transactions on. 2008;16(5):479–484.
17. Amick RZ, Chaparro A, Patterson JA, Jorgensen MJ. Test-Retest Reliability of the SWAY Balance Mobile Application. Journal of Mobile Technology in Medicine. 2015;4(2):40–47.
18. Patterson JA, Amick RZ, Thummar T, Rogers ME. Validation of measures from the smartphone SWAY Balance application: A pilot study. Int. J. Sports Phys. Ther. 2014;9(3):135–139.
19. Chakraverty R, Pynsent P, Isaacs K. Which spinal levels are identified by palpation of the iliac crests and the posterior superior iliac spines? J. Anat. 2007;210(2):232–236.
20. Zephyr BioHarness 3. 2014; http://zephyranywhere.com/products/bioharness-3/. Accessed October 2nd, 2014.
21. Le Clair K, Riach C. Postural stability measures: what to measure and for how long. Clin. Biomech. 1996;11(3):176–178.
22. Yu E, Abe M, Masani K, et al. Evaluation of postural control in quiet standing using center of mass acceleration: comparison among the young, the elderly, and people with stroke. Arch. Phys. Med. Rehabil. 2008;89(6):1133–1139.
23. Moe-Nilssen R, Helbostad JL. Trunk accelerometry as a measure of balance control during quiet standing. Gait Posture. 2002;16(1):60–68.
24. Day B, Steiger M, Thompson P, Marsden C. Effect of vision and stance width on human body motion when standing: implications for afferent control of lateral sway. The Journal of physiology. 1993;469:479.
25. Amiridis IG, Hatzitaki V, Arabatzi F. Age-induced modifications of static postural control in humans. Neurosci. Lett. 2003;350(3):137–140.
26. Duncan PW, Studenski S, Chandler J, Bloomfeld R, LaPointe LK. Electromyographic analysis of postural adjustments in two methods of balance testing. Phys. Ther. 1990;70(2):88–96.
27. Horak FB. Clinical assessment of balance disorders. Gait Posture. 1997;6(1):76–84.
28. Horak FB, Nashner LM. Central programming of postural movements: adaptation to altered support-surface configurations. J. Neurophysiol. 1986;55(6):1369–1381.
